As I mentioned previously, I have determined Qigong is the form of Yoga that I intend to do as part of my exercise protocol to minimize Parkinson’s symptoms. I have included excerpts from the newsletter with helpful information about the routine. To read the entire newsletter, it may be found at taichi18.com
In this newsletter, I would like to address some frequently asked questions and common mistakes made by students when they practice the shibashi qigong. Frequently Asked Questions (Part I):Q.What is the ideal speed of doing this qigong? A. The ideal speed for each person is different. The speed should depend on your own breathing since each movement is coordinated with breathing. If your breath is shallow, you may tend to perform the whole set faster than if your breath is deep.Beginners who have no previous training in breathing usually perform the whole set in about 10 minutes. That is about 12 breathes per minute. In my videos, I performed the set in this pace since I assumed most viewers were beginners. After you remember all the movements and their sequence by heart, you should do it at your own pace, no need follow the pace of the video anymore. When I practice this qigong on my own, I usually spend about 20 minutes to perform a set. That is about 6 breathes per minute or 0.1 Hz (cycle per second). Coincidentally, it makes scientific sense to perform the Shibashi at this pace. …………..Studies have found that there are many positive effects both physically and emotionally when our bodies vibrate at this resonant frequency.For human beings, the resonant frequency of our system is approximately 0.1 Hz…………………………Most people should be able to perform the Shibashi at a pace of 6 breaths per minute (0.1Hz), after practicing daily for a couple of months. Again, doing the exercise at a comfortable pace is more important than trying to achieve 6 breaths per minute……………..
Q.What is the benefits of each movement? ……………..Just remember, the whole is greater than the sum of its parts.
Q.Can I increase the number of repetitions for each movement? A. It would be more beneficial to do the entire set twice instead of increasing the number of repetitions for each movement. However, if a particular movement makes you feel really good, you could repeat that movement a few more times.
Q.How often should I practice this qigong? A. You may do it as often as you like. However, I’d say do the entire set twice in the morning and twice in the evening is enough. ………………
Common Mistakes – Shoulders:
Most beginners tend to raise their shoulders when they raise their arms. The shoulders should be relaxed all the time because when they are relaxed, you can breathe deeper, thus allowing the whole body to be more relaxed. Also, the qi flow to the arms would be much better when the shoulders are relaxed. Sadly, many beginners are often so tense and stressed out that they forget how to relax their shoulders.
Here is a simple technique to relax the shoulders:
a. Breathe in, raise the shoulders. b. Hold the breathe for 10 seconds, hold the shoulders in the raised position. c. Breathe out, let the shoulders sink down naturally.
Repeat steps a – c at least 9 times. There is a free video clip on https://taichi18.com/online-video-course/shibashi that talks about how to check and make sure your shoulders and relaxed during the movements.
PERHAPS I can have an opportunity to participate in this one, too???
“The progress of MCC950 to market appears to be happening rather quickly. Both the Michael J Fox Foundation for Parkinson’s Research and the Ireland-based drug company Inflazome are keen for human trials to start as soon as possible.
Dr Woodruff said much of the preclinical work was already completed.
The biggest hurdle, apart from funding, is that MCC950 came off a patent. This means the researchers have had to develop variations of the original drug for intellectual property reasons. Those new drugs are currently being tested and, according to Dr Woodruff, proving to be even more effective.
There are 10 million people with Parkinson’s disease worldwide. They still have a few years to wait and see if the magic in the lab can be replicated in people.
The phase-one tests next year will determine whether or not the drug is safe in healthy people. All going well, volunteers with Parkinson’s will be recruited for phase-two testing in 2020.
Whether Michael J Fox himself will be one of those volunteers is not yet known.”
Dr. C’s Journey with PD – a column by Dr. C from: Parkinson’sNewsToday.com
I hate exercise! Both my pain and fatigue increase when I exercise. These are disabling Parkinson’s disease symptoms, and both trigger the fight-or-flight response that often manifests as “the grouch.” I have not found an easy way of exercising with Parkinson’s pain and fatigue, but I have found ways to shift my perspective. Shifting perspective opens up the possibility of experiencing enjoyment from exercise.
One of the most important parts of a Parkinson’s wellness map is exercise. But here’s the catch: It’s difficult to do with regularity. We know it works! Yet, knowing what is good for wellness is not the same as doing it. The doing part of exercise — showing up three to four times a week — is difficult with all the chronic disease barriers. It’s easy to feel defeated before even starting.
The way around this apparent Catch-22 is to shift one’s perspective on exercise. I mentioned the idea of shifting perspective in connection to wellness in a column about moments of well-being. The shift I need with regard to exercise is one that will get me off the sofa and into exercising. I am not getting off the sofa to do something I hate, but rather to do an enjoyable, creative project that involves exercise: landscaping to produce gardens. It’s a good exercise to keep the trunk strong, which helps prevent falls.
It takes a bit of perseverance to get into my work clothes, strap on the heavy work boots, find the hat and sunglasses, and then head out the door. Surveying the work ahead — which is sometimes a bit daunting — I start with light work to warm up. Walk, then shovel, and maybe rake, before getting behind the wheelbarrow to move gravel or dirt from one location to another. Pause to hear the birds sing, marvel at the variety of flower blooms and fragrances. Pretty quickly, the world slips away, replaced by the Zen of gardening.
My Fitbit reminds me when a time for medication is coming up and keeps track of my heart rate. I take lots of water breaks! By the time two hours have passed, my work shirt is drenched with sweat — as much as, if not more than, the amount of water I’ve consumed. In the Zen garden moments, the mind is free of the worries of Parkinson’s and vision problems. That feeling remains with me, not as a false euphoria, but as a deep-rooted sense of well-being.
There are many ways that shifting perspective can open wellness possibilities. A nurse shared a wonderful example. She was a smoker from her early teen years, and now in her 30s, she decided to quit. Six months without a smoke and she says, “I had this memory of how much I enjoyed smoking.” So, she bummed a cigarette and immediately got sick from smoking it. Recounting the event, she says, “I can remember the horrid feeling as clear today as if it just happened. I never had the urge to smoke again after that.” She shifted her perspective from enjoying smoking to thinking of it as a horrid, sickening experience. Shifting perspective opened up the possibility of wellness.
The ability to shift perspective may also improve our ability to adapt to stressful times and to become more resilient, and therefore more open to new possibilities. The shifting of perspective causes us to shift our focus to a new intention, a new possibility. I hated exercise, and my intention was to avoid it. The shift in perspective offered the new intention of enjoyment and the possibility of a beautiful garden, along with a healthier body, in spite of the chronic disease limitations.
The following photo is a visual description of how I feel my participation in conversations go. When someone asks a question, so many variations of a response are running around in my head, by the time I decide which response I want to make, the conversation has moved on, and my comment goes unvoiced. (I think it might be related to the bandwidth referenced below)
I am finding… when I focus on taking larger strides, challenge myself to go swiftly up the stairs at the temple, instead of using the elevator, follow my to do list, for gardening, breathing exercise, etc..and go out of my way do a service project each day… the intentional INTENT truly goes a long way.
Below are excerpts I have taken from conversations in an online Parkinson’s community, that alludes to the variety of physical skills effected… and TEACH us how, with INTENT we can keep functioning.
…………………………………..
David L educated us : “Walking backwards worked because you had to use INTENT. Intent is the key to everything related to Parkinson’s. Dopamine is responsible for the smooth operation of the things we do “automatically”, like swinging your arms when you walk, taking a deep breath before you speak, making your tongue do its thing for speech and swallowing, getting words from your brain to your mouth, and on and on. By the time of diagnosis a PLWP has already lost 80% of the cells that produce dopamine. When intent is implemented, we are able to bypass the “automatic” track of the brain, which requires dopamine, to a non- automatic track. One must really think about walking backwards lest one stumble and fall
………………………………………
lowreyjw said: …… “I have breathing problems similar to yours – if what I have noticed is true, then it has something to do with PD weakening the diaphragm and lessening the power of activity.
I am taking breathing therapy and the net effect is to strengthen the muscle tone and power of diaphragm response when inhaling and exhaling – I notice my breathing is shallower rather than weaker, and if I take extra effort my lungs inflate just as they did before PD – but I have to think about it, possibly another case of the neural bandwidth narrowing…
What follows was written by Omotola Thomas. Funny and sad at the same time. She has had PD longer than I, and her frustrations are showing.
Typing under the influence of Parkinson’s: 3 things your doctor didn’t tell you.
1. Typing will suck! Don’t try to fight it…. it will progressively suck! Did I just hear you say “Well, I can just use voice-to-text“? Sorry to burst your bubble, but as your voice gets weaker with PD, so will the ability of the V2Txt to decipher what the heck it is you are trying to say. If, like me, you are prone to ending your messages with “xx” to indicate the 😘 emoji, your precious dirty-mind of a V2Text-er will instead type “sex sex“… And when, in horror, you hurriedly try to delete it, your tremoring fingers will accidentally hit “send“. Imagine meaning to type “Cool… Let me know if you want to do it xx” 🥺🥺🥺
2. When you see your friend’s distraught Facebook post about her dog that just died, you will try to show your sympathy by clicking the “😢” emoji, but instead, you will click the “😂” emoji , and each time you frantically try to change it, you will re-select “😂”. If you are wise, you will accept your fate and stop trying because if you continue, somehow… (and I cannot explain how) the next thing that will happen is that you will end up “activating” and inadvertently sending a highly inappropriate GIF. The frustrating thing is that when you do actually want to send a GIF, you will not know how to. 🤦🏾♀️🤦🏽♀️🤦🏽♀️
3. When someone sends you a WhatsApp message, and you proceed to respond … They will see (on their end) that you are “…..typing”. They will see this “ …..<insert your name> typing” for a very long time, which will indicate to them that they are about to receive a long message from you. imagine their irritation when, after staring at “…is typing” for 6 1/2 minutes, your reply comes in and all you have managed to type is “Ok. Got it 👍🏾. “ 😐😐😐
One of the on-line communities I enjoy has each person answer questions, as a way to introduce themselves. I share this information, in the for what it is worth… (sounds like more assistive for dementia)
………………………………to the phrase to be completed ….. …… Given what I know now, I would recommend others...
Totally avoid insecticides. They affect the nervous system not only of insects but of us too. As far as I know, PD isn’t fatal, but the accompanying Alzheimer’s/dementia is what kills us. Good news – My favorite herb book, The Way of Herbs by Michael Tierra, C.A., N.D. pub by Pocket Books, 1990 p. 170 states: “In Europe, several studies were made on geriatric patients. According to herbalist Amanda McQuade, ‘one study of patients between the ages of 60 and 80 with senile dementia showed measurable improvement in as little as eight weeks. Treatment with gingko under four to eight weeks is considered too short to be effective. No side effects or habituation have been demonstrated using the average dose of 40mg, three times daily, for three months. Even a single dose of 600mg given experimentally to young women produced no side effects except improved memory.’ Source: Amanda McQuade, “Strange and Beautiful Gingko” Let’s Live vol. 56, #5, (June 1988), pp. 80-83.” I have used it myself, and enjoy the lasting effects even though I have finished my 8 weeks of supplementation. I have started taking it again recently to avoid cognitive impairment. Be picky if you buy some. Read the label for additives such as rice powder & beeswax. The only ingredient should be powdered ginkgo herb & the capsule. Enjoy your beautiful mind!
………………….. and a different perspective…. from the conversation…
“It didn’t just work for me, but for Alzheimer’s/dementia residents in a study in a nursing home in Europe that I read about in my herb book. I could only find 60 mg capsules here, so took twice a day with good results. I found some herbal companies added beeswax, rice powder etc, so I started looking for brands that contained only the herb plus the capsule. Lots of times I skipped the capsule, and opened it & poured it on applesauce. A chiropractor once told me that if your body needs something, it tastes good to you – it does to me. Before I took a pre-DBS psychoneurological test, I took 120 mg all at once. The neuropsychologist was very impressed with my test results, He said there were parts of the test he had never administered before, because no one could get that far on it. It works! And I stopped after 6 months.”
I think YOU SHOULD LIKE THIS… Sarah, of Invigorated, shares these 4 strategies… (link to entire article is below the recipes)
“It’s no surprise that the hunt is on for new therapeutic approaches for Parkinson’s that target the gut microbiota (10-12). Fortunately, you don’t have to wait for the next scientific breakthrough to get a jump start on improving the health of your gut.
The goal of this jump start is to begin to decrease inflammation, heal the gut lining, and restore healthy gut balance (good and bad bacteria) through 4 simple strategies that you can start today with very little investment and very little change to your diet.
Let’s take a look…
#1. Add a Digestive Detoxifying Elixir (upon waking)
An easy way to prepare your gut for the day is to drink a combination of raw apple cider vinegar (ACV), lemon, and warm water first thing in the morning on an empty stomach.
Raw apple cider vinegar is a scientifically proven antifungal, helps stabilize blood sugar, and stimulates digestion while lemons are high in Vitamin C. These help kick-start the detoxification of the liver, allowing it to produce bile and move toxins into your stool.
Combine and chug. (Plugging your nose helps with the bitterness!) Swish some water around your mouth and teeth after to help with the taste and protect your tooth enamel.
#2. Hydrate Properly (within 30 minutes of waking)
Hydrating properly early in the day will stimulate your digestion and help your body flush out toxins that have accumulated while you were sleeping. Adding a pinch of celtic sea salt to your water helps you hydrate efficiently, as well as nourish your adrenals and balance your blood sugar. Drinking a water bolus (at least 16 ounces in one sitting) can also boost blood pressure if you have a tendency to run low in the morning (16).
Combine and drink at least 16 ounces. Do this before having any caffeine. Drink the second 16 ounces within the hour.
#3. Take a Power Walk (before 10AM)
Exercise stimulates digestion, and walking specifically produces a wringing motion in your torso that helps detoxify and move food along your digestive tract. When you walk early in the morning, the sunshine hitting your eyes helps regulate your circadian rhythm and lets your body know it’s time to wake up.
Take a 10-15 minute power walk around the block. Emphasize swinging your arms, or use walking poles for added benefit.
#4. Eat a Healthy Breakfast (first meal of the day)
The first meal of the day should be packed with nutrients, fiber, and antioxidants needed for gut healing and building a balanced gut microbiome. Eating “brain-boosting” foods like fresh fruits and vegetables, healthy fats, nuts, and seeds will also keep your blood sugar balanced so you have more energy throughout the day.
Aim to have the first meal of the day be the healthiest, and ride the wave of success the rest of the day!
Here are 3 “brain-boosting” breakfast options to try this week that take minimal preparation.
POWER BOWL
¼ large avocado, sliced
2 boiled eggs, cut in half
2 cups of green kale, torn up by hand
⅓ cup sauerkraut*
2 Tbsp organic coconut oil
Pinch of celtic sea salt
Pinch of ground pepper
Add kale and coconut oil to a skillet over low-medium heat. Sautee, stirring occasionally until kale softens. Sprinkle with celtic sea salt and remove from heat.
Add avocado, egg, and sauerkraut on top.
Enjoy!
*Skip the sauerkraut if you are taking an MAO-B inhibitor which does not react well with fermented foods.
I am posting this just prior to the four strategies for gut health… You should see why. 🙂
You may recall from an earlier post: STUDY PURPOSE: The most urgent unmet medical need in Parkinson’s disease is a treatment targeting the underlying disease mechanism and thus prevent the disease from progressing rather than only controlling symptoms. The study drug tested in this study is a new chemical compound called UCB0599, which could have such effects by preventing the aggregation of alpha-synuclein in the brain, which is thought to be the main driver of the disease progression.
Since the alpha-synuclein is the focus of our current clinical trial… I found the following to be of great interest.
Notes from the convention as passed on by Laura Kennedy Gould’s Blog : THE MAGIC TRICK-Life With Parkinson’s
Alpha-Synuclein in your gut
I attended a technical lecture about alpha synuclein (A-syn). Since the last congress three years ago, A-syn has been found in the appendix. Apparently, a-syn spreads from the appendix to the gut and by the vagus nerve to the brain. Different shapes of a-syn aggregation have been identified with each representing a different disease – i.e. PD (spaghetti), ALS (ribbon fibril) or MSA (linguine). These aggregates form Lewy bodies. The scientists have discovered that a-syn connects with 178 proteins; however it is not yet known if any of these cause PD or are a result of it. What I gather from this is that the researchers have learnt a lot but are no closer to finding a cure. Additional testing and research is needed to further define the role of a-syn and Lewy bodies in relation to PD.
Although I tried the Keto diet, for 9 months, in an attempt to get more good oil to my brain, I understood it should not be my permanent new lifestyle. The results of all my testing, here at the clinical trial indicate (other than my Parkinsonism symptoms) I am VERY healthy….
What follows is a very comprehensive report detailing the study results and the time line for the evolution of diet trends and results through the years… Taken from https://medium.com/@KristenHovet/
………I thought the information was helpful….for my peace of mind……….
………..”The results from new and pooled research on low carbohydrate diets were presented at the European Society of Cardiology’s 2018 Congress in August by researchers based in the UK, Poland, Sweden, and Greece. The findings are not good for those following low carb diets.
To carb or not to carb? That has been the question, and the source of several polite (and not-so-polite) conversations with friends, family, and random strangers online. And the answer, at least according to the study in question, is a resounding to carb!
The researchers concluded that low carbohydrate diets are unsafe and should therefore not be recommended to patients. There is a small subset of patients for whom low carb diets are likely beneficial, but physicians cannot in good faith recommend low carb diets to the average individual who is seeking to lose weight or maintain weight. Low carbohydrate diets can indeed be effective for weight loss, but they do not appear to be suitable — or safe — for the long-term.
And though ketogenic and other low carb diets have been popular for several decades, particularly with those looking to shed a few pounds, cutting carbs has remained controversial to doctors and health experts alike. At the peak of the low carb diet craze in the late 1990s and early 2000s, nearly 20 percent of the American population was estimated to be following a low carbohydrate diet of one form or another.
Previous studies have been in short supply, and those available have been inconclusive or incomplete. Regardless of the paucity of comprehensive research, several “health gurus”, nutritionists, dieticians, naturopaths, and even medical doctors around the world have spent a great deal of energy and time promoting ketogenic and low carbohydrate diets to the general public. Some have made their fortunes this way. The sheer number of books and articles written on the subject speaks to the popularity of the low carb movement.
The study we’re exploring today could mark the first in a series of critical blows about to hit the low carb and keto communities. Due to the size of the cohorts in the experiments reviewed and due to the length of time the individuals were followed, the results are particularly convincing.
Study author Maciej Banach, of the Medical University of Lodz, Poland, said: “We found that people who consumed a low carbohydrate diet were at greater risk of premature death. Risks were also increased for individual causes of death including coronary heart disease, stroke, and cancer. These diets should be avoided.”
The researchers looked at the relationship between low carbohydrate diets and all-cause mortality, as well as death due to cardiovascular disease, cerebrovascular disease (e.g. stroke), and cancer. Their research subjects were part of a large and nationally representative cohort of 24,825 Americans, and study data was collected from the National Health and Nutrition Examination Survey (NHANES), covering the years 1999–2010. The mean age of participants was 47.6 years old, and the cohort was 48.6 percent men and 51.4 percent women.
Image: Eiliv Sonas Aceron
Participants who had the lowest carbohydrate intake had a 32 percent higher risk of all-cause mortality over an average of 6.4 years follow-up, while the risk of mortality due to cardiovascular disease, cerebrovascular disease, and cancer increased by 50 percent, 51 percent, and 35 percent, respectively.
The researchers then performed a meta-analysis using seven prospective cohort studies. The meta-analysis validated the scientists’ own findings, and taken together included 447,506 participants.
“We showed that subjects in the top quartile (those with the lowest intake of carbohydrate) had the highest risk of total mortality,” the researchers said. Additionally, they found a significant link between low carbohydrate/high protein diets and cancer mortality. The research team notes that further studies will clarify the mechanisms behind these associations.
The take-home message: Unless you have a particular medical condition that has evidence-based and well-documented reasons for following a long-term low carbohydrate diet, it is best to avoid low carb and ketogenic diets altogether. Stick with balanced diets rich in healthy carbs, like whole grain breads, buckwheat porridge, sweet potatoes and yams, and blueberries — to name just a few.
Low carb diets have been around for quite a long time, and the first formulations were also linked to health and weight loss. Here are some of the key players that have contributed to our long-standing obsession with low carb diets (an obsession that may be on its way out):
1863–1869: William Banting promotes a low carb diet for weight loss and health, based on his own success losing weight.
1921: Low carbohydrate diets are used to treat paediatric epilepsy. These diets can still be used today for some children who do not respond to medication, but in most cases medication is preferred.
1927: Explorer and ethnologist Vilhjalmur Stefansson promotes an Inuit diet, based on the diets of Inuits in Iceland and Canada. In today’s terms, we would consider this a “zerocarb” or “extreme keto” approach.
1935: Though suffering from a serious lack of evidence, the alkaline diet is all the rage. Many carbs and starchy foods are thought to be “acid forming,” and must therefore be avoided.
1967: The Stillman diet is created by Dr. Irwin Maxwell Stillman. It is a kind of “proto-Atkins diet,” with a focus on low carb and high protein ketogenic eating. The Stillman diet promotes six small meals a day.
1972: Dr. Robert C. Atkins publishes “Dr. Atkins’ New Diet Revolution,” kicking off the very popular Atkins diet trend. Robert Atkins is said to have died from a fall that occurred nine days prior to his death (at the age of 72), but a medical report showed that he had clear signs of having suffered a history of heart attacks, congestive heart failure, and high blood pressure.
1975: Walter L. Voegtlin publishes “The Stone Age Diet.” The advice is to “eat like a caveman” — a diet high in meat and seafood; with moderate fruit and vegetable intake; and very low or no grains, dairy, or added sugar or salt.
1985: Stanley Boyd Eaton and Melvin Konner publish a paper called “Paleolithic Nutrition,” which supports Voegtlin’s Stone Age diet. 2002: The Stone Age diet makes a comeback in the form of “The Paleo Diet” by Loren Cordain, founder of the Paleo Movement.
2003: Dr. Arthur Agatston publishes “The South Beach Diet.” The focus is on foods with a low glycemic index (GI) and low glycemic load (GL).
2015: Dr. Michael Mosley publishes “The 8-Week Blood Sugar Diet.” It’s a low carb, Mediterranean style diet that includes optional intermittent fasting and ultra low calorie options. The blood sugar diet is promoted for those at risk of developing Type 2 diabetes or for those who have already been diagnosed with diabetes or metabolic syndrome.
Ketogenic diets regain popularity and are marketed for weight loss purposes. The trend continues to this day.
This timeline has been adapted from the Diatetically Speaking website by Maeve Hanan.
Not all people with Parkinson’s disease experience the same symptoms. For example, I am most affected by bradykinesia, poor fine motor skills, incontinence, and fatigue.
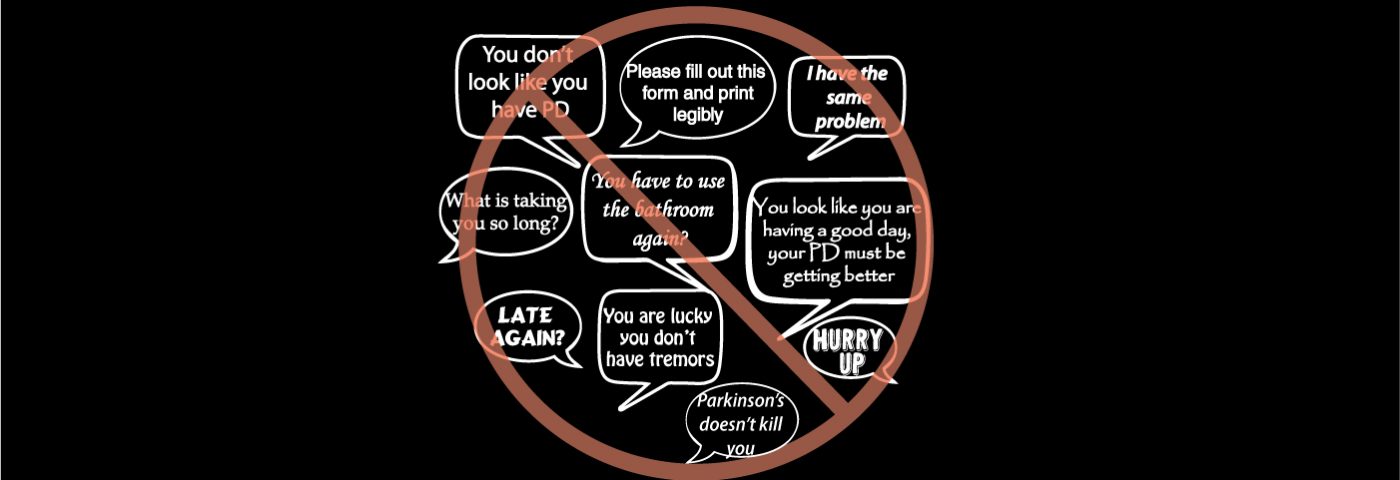
I was inspired to write this column based on my personal experiences after I read Sherri Woodbridge’s column, “What to Say to Someone with Parkinson’s Disease.” Most people don’t know what to say and usually have good intentions. However, poorly chosen words can break a person down. Be mindful of how you speak to someone with Parkinson’s.
“Words can inspire. And words can destroy. Choose yours well.” —Robin Sharma
1. ‘You don’t look like you have Parkinson’s.’
This is my least favorite comment. Many of my symptoms are unseen. People have no idea how much I am struggling at times to maintain some semblance of normalcy. Most days, I feel shaky and weak, and I am totally exhausted.
A comment like this can minimize the hidden symptoms that are very real to the person with Parkinson’s. Most people do not understand what those of us with the disease deal with daily and sometimes hourly.
2. ‘You are lucky you don’t have tremors.’ Or, ‘Your symptoms could be worse.’
Parkinson’s is progressive and unpredictable. It’s impossible to know where my symptoms might be six months from now, let alone six years from now. Just because I don’t exhibit a particular symptom now does not mean I will never have it. At times, Parkinson’s feels like the sword of Damocles hanging over my head.
3. ‘You look like you are having a good day. Your Parkinson’s must be getting better.’
If I am having a good day with few symptoms, it doesn’t mean that my disease is getting better. There is no cure and no way to heal from Parkinson’s. For me, good days are fleeting and the exception to the rule. A comment like this serves only to remind me that Parkinson’s is progressive.
4. ‘I have the same problem.’
Sometimes, people respond with this statement when I comment about one of my symptoms (choose any of the following):
tripping
having to sit down when I put on my shoes
losing my balance all the time
forgetfulness
inability to multitask
I think well-meaning people say they have the same issues because they don’t want me to feel alone in experiencing these challenges. After all, they can develop over the natural course of aging. Most people do not understand, however, that I used to be very sharp mentally and was a strong athlete and dancer before I was diagnosed. That makes these symptoms much more glaring for me.
5. ‘Hurry up!’ Or, ‘What is taking you so long?’ Or, ‘Late, again?’
With Parkinson’s, I have two speeds: slow and slower.
I clearly remember, years ago, watching my Parkinson’s-diagnosed friend putting on her coat or fastening her seat belt. I would think to myself, “Why is she so slow?” Now, I totally understand what she was dealing with.
6. ‘You have to use the bathroom again?’
My late husband always told me my life was ruled by my bladder. No truer words have been spoken, especially now that I have Parkinson’s. I never like to be too far from a bathroom. I found a smartphone app called Flush that displays public restrooms nearby, and I never leave home without it!
7. ‘Please fill out this form and print legibly.’
Doctor’s office staff, please take note of this one. I cringe whenever I see a new doctor and have to fill out reams of paperwork. My handwriting is atrocious; it was the first symptom that sent me to the neurologist. And guess what? I had to fill out a lot of paperwork at his office! Although my typing on a computer is no longer as fast as it used to be, at least I have a spell-checker. E-forms are a greatly appreciated and preferred option.
8. ‘Parkinson’s doesn’t kill you.’
It’s true that people do not die from Parkinson’s, but they typically die from complications of the disease. As an example, Parkinson’s can impair patients’ ability to swallow, putting them at risk for inhaling, or aspirating, food or liquid into their lungs, leading to aspiration pneumonia. Pneumonia is the leading cause of death in patients with this disease.
Still, I fear living with a poor quality of life and loss of my independence more than I fear dying.
In the grand scheme of things, comments made out of ignorance are no big deal considering what people with Parkinson’s deal with every day. Now that you know what not to say, read Sherri’s column on things you can say to someone with Parkinson’s.
“Sometimes you don’t have to say anything. Silence speaks it all.” —Disha Patani